Medical Treatment Options for Fibroids: What You Need to Know
By Moona Arabkhazaeli, MD
Minimally Invasive Gynecologic Surgeon
Who needs treatment?
As discussed in the introductory fibroid blogpost, fibroids are very common. In many cases they are small and asymptomatic, and therefore treatment is not necessary. Instead, the fibroids can be monitored with an annual exam.
Understanding Your Treatment Options: Medical Options and Surgical Options
As I note below, there are both medical and surgical options for the treatment of fibroids. In this post, I'll be describing your medical treatment options. Watch for my next article about surgical options.
Two Categories of Symptoms
If fibroids are symptomatic treatment is warranted. There are two categories of symptoms that can result from fibroids.
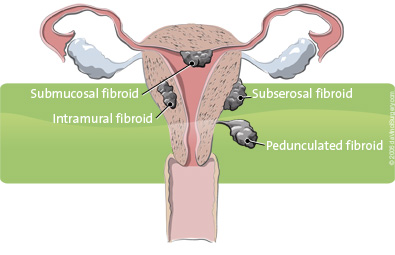
The first is abnormal uterine bleeding - this refers to heavy, and often painful periods. There is no strict definition of what constitutes a "heavy period," rather, it's best to trust the patient's perception of what they consider heavy. Whether fibroids are going to make periods heavy depends on their size and location; submucosal fibroids, those that are located along the endometrial lining, are most likely to result in bleeding symptoms.
The second category of symptoms is referred to as bulk symptoms. These arise from the sheer size/weight of the fibroids, and include pelvic pain, pelvic pressure, and urinary frequency or retention.
Fibroids can also be implicated in infertility but that topic warrants its own blogpost!
How do I decide between medical or surgical treatment?
The best type of treatment depends on your treatment goals, what symptoms are present, and the size, number and location of fibroids. Each treatment course is very individualized, and I encourage you to talk to your doctor about the pros and cons of each, and what would work best for you.
In general, medical treatment tends to be favored for people to have bleeding symptoms rather than bulk symptoms. This is because medical options work to slow down the menstrual flow associated with fibroids, but do not eliminate or significantly shrink the fibroids themselves. For this reason, if someone has bulk symptoms due to fibroid size, surgical treatment may be a better fit. The one exception to this is GnRH analogs (discussed below); these are medications that can shrink the size of the fibroids, but only in the short term.
So what are the options for medical treatment?
Combined estrogen-progestin contraceptives: These come in the form of a pill, patch, or ring, and known as traditional "OCPs." They are usually the first line approach, as can be used long-term, are well-tolerated, are relatively inexpensive, and provide contraception and additional benefits including decreasing the risk of ovarian and endometrial cancers.
Progestins: Options include high dose oral progestins (norethindrone acetate or medroxyprogesterone acetate most commonly), a progestin injection ("Depo provera," administered every 6 months), the etonorgestrel arm implant ("Nexplanon"), or the levonorgestrel intrauterine device (IUD). However, there is compelling evidence that the progesterone IUD results in a greater decrease in menstrual blood loss as compared to oral or other routes of administration. One factor to note with progestins compared to OCPs is that while CHCs maintain a regular menses, continuous progestins can suppress periods completely (ie amenorrhea) or result in irregular bleeding. While this does not have negative long-term consequences (owing to its mechanism), it may be bothersome for some.
Gonadotropin-releasing hormone (Gn-RH) agonists and antagonists: These drugs block the production of ovarian-stimulating hormones, lowering estrogen levels. Since fibroids are estrogen responsive, this results in reduction of menstrual bleeding, and notably, some reduction in fibroid size. Because these drugs create an artificial menopause, one often experiences menopausal side effects such as hot flashes, sleep issues, and vaginal dryness. Some of the newer oral options mitigate this by including a low dose of estrogen and progestin added back within the medication. There are currently two oral Gn-RH agonists on the market that are FDA approved for fibroid related heavy menstrual bleeding - Myfembree (relugolix-estradiol-norethindrone) and Orianhh (elagolix-estradiol-norethindrone). These medications have been found to result in a 50% reduction in menstrual blood loss, and can even improve bulk symptoms. However, due to limited data at this point they are both only approved for up to 24 months of use, and are not approved to be used as a contraceptive.
Tranexamic acid ("Lysteda"): This is a non-hormonal medication that works to slow down the breakdown of blood clots. In turn, slows down bleeding, and in this case can be used to reduce fibroid related bleeding. It is only taken during your period, rather than the entire month, and is non-hormonal; this makes it a good option for those who prefer to avoid contraception or a daily medication!
Topics
Share this page:
About the Author
Moona Arabkhazaeli, MD
Minimally Invasive Gynecologic Surgeon
 Dr. Moona Arabkhazaeli brings specialized expertise in Minimally Invasive Gynecology Surgery to her role at Minnesota Women's Care. Her dedicated focus lies in areas such as abnormal uterine bleeding, endometriosis, pelvic pain, and fibroids. Dr. Arabkhazaeli's expertise extends to minimally invasive surgical techniques, which optimize patient outcomes by reducing complications and expediting recovery. With a patient-centered approach, she emphasizes compassionate and personalized care, aiming to empower women in their healthcare journey. Dr. Arabkhazaeli's dedication to innovation and her proficiency in minimally invasive techniques underscore her commitment to delivering optimal outcomes for her patients.
Dr. Moona Arabkhazaeli brings specialized expertise in Minimally Invasive Gynecology Surgery to her role at Minnesota Women's Care. Her dedicated focus lies in areas such as abnormal uterine bleeding, endometriosis, pelvic pain, and fibroids. Dr. Arabkhazaeli's expertise extends to minimally invasive surgical techniques, which optimize patient outcomes by reducing complications and expediting recovery. With a patient-centered approach, she emphasizes compassionate and personalized care, aiming to empower women in their healthcare journey. Dr. Arabkhazaeli's dedication to innovation and her proficiency in minimally invasive techniques underscore her commitment to delivering optimal outcomes for her patients.
If you or someone you know is experiencing the symptoms of uterine fibroids, visit mnwcare.com or call 651-600-3035.